
Overtraining Syndrome in the Athlete
What is Overtraining Syndrome
Overtraining occurs when training stimulus or workload is too high for the body to tolerate, resulting in decreased performance and increased risk for injury or illness. Clinically, overtraining syndrome refers to a disorder of the hormonal and nervous system that occurs in response to accumulative fatigue from excessive training and /or inadequate recovery.

Basically - an athlete reaches their ‘tipping point’ after prolonged exposure to elevated stress and exercise demands.
Not to be confused with over-reaching, which can also present with some mild physical and/or psychological symptoms, but is a more short-lived , transient state that resolves with short periods of rest and recovery based exercise. Over-reaching is usually an intentional process of increasing training load/intensity in aims of eliciting a “Super-compensation” effect in lead up to competition. Super-compensation is simply a short-term performance enhancement response following a big spike in training load above normal levels (i.e. over-reaching phase).
For most of the general population, overtraining is not a huge risk unless undertaking aggressive increases in exercise frequency/intensity/duration/compexity.
Overuse injuries, on the other hand, are common in response to prolonged high intensity training or un-accustomed physical activity - but for this article, overtraining will refer specifically to the presentation of overtraining as a syndrome with more severe physical and psychological symptoms (lasting >2 months).
What are the main risk factors ?
Overtraining is multifaceted, and many factors can both directly and indirectly contribute to any athlete’s risk for overtraining.
Rapid and unaccustomed increases in workload (intensity, number of sessions, duration or task complexity etc)
Extended periods of high workload training without a break
Extended periods of monotonous training with little or no variation
While factors contributing to overtraining are important, there are also risks associated with ‘under-recovering’.
Under-recovery may be overlooked when following a seemingly well-written training program. The demands of elite performance training are high, and the ability to tolerate these demands involves taking measures to optimise how the body recovers.
This may include methods such as massage, cold/ice bathing, stretching etc. (*check out our intro recovery blog for more detail), however the simplest methods involve adequate rest and nutrition - which should be planned into/around a good sports performance or fitness program.

The other area of risks includes external factors such as environmental stressors. This ties in closely with under-recovery because the bodies capacity to tolerate high demands is reduced when there are added work/study/family stress (in addition to anxiety of impending competition, concerns around training performance and fear of failure).
All these factors can contribute to cycle of poor sleep/rest and inadequate recovery, as well as heightened stress responses to usual training demands - leaving the body in a compromised state.
What happens to the body?
Now we have an overview of the factors that may lead into overtraining syndrome - but what’s actually happening to the body?
There are many signs and symptoms that could lead to suspicion of overtraining syndrome.
Physiological variables that are important include:
Persistent fatigue
Persistent muscle soreness/tenderness
Loss of body mass and altered body composition
Decreased effort-economy and lactate threshold at given workload
Reduced performance despite continued progressive training
Cardiovascular changes such as increased early morning heart-rate or blood pressure
Haematology changes (such as reduced serum Ferritin)
Hormonal changes (such as decreased catecholamine production or changes to testosterone : cortisol ratio)
Frequent illness (such as Upper Respiratory Tract Infection)
Research has identified a handful of areas that are consistently altered in athletes with overtraining syndrome.
Performance reductions
Persistent high fatigue ratings
Reduced maximal heart rate by 5-10bpm
Changes in blood lactate concentration and lactic threshold at given workload
Elevated resting plasma stress hormones, such as adrenaline/epinephrine with decreased noradrenaline/norepinephrine
High self reported stress levels and sleep disturbance

Hormonal Response
Hormones that are thought to be affected include Testosterone and Cortisol. Testosterone is known to support androgenic-anabolic (growth & repair) activity while Cortisol support catabolic (breakdown & consumption) activity.
Resting Cortisol levels haven’t been proven in research to be elevated but maximal cortisol secretion is reduced in the overtrained athlete.
Circulating Testosterone has also been found to be reduced in the overtrained athlete but there aren’t really any strong evidence based findings around this.
The ratio of Testosterone to Cortisol has been suggested to be a valid marker of overtraining (and potentially a diagnostic tool) - given that Cortisol and Testosterone have opposing effects on skeletal muscle growth, protein synthesis and metabolism.
A decrease of Testosterone : Cortisol ratio of 30% is suggested to be indicative of overtraining syndrome in the athlete. Again, given the inconsistency of good quality research to support this - the recommended method of frequently monitoring the ratio over time is not yet something that is done commonly.
Immune System Response
Immune system changes are also thought to occur in overtrained athletes, although there isn’t a great deal of research to actually demonstrate many physiological changes.
Neutrophils (one of the key white blood cells of the immune system) have long been implicated in illness/infection risk particularly in response to chronic stress and inflammation. While studies have found higher neutrophil counts in response to increased exercise/training load, there isn’t
Salivary ImmunoGlobulin A (IgA) has been measured in overtrained and healthy athletes who are well trained, with clear reductions seen in the overtrained. Studies have also suggested that monitoring Salivary IgA can be a useful tool to detect risk for overtraining.
Plasma glutamine (an important mediator of immune cell function) concentrations are shown to decline in overtrained athletes, however there hasn’t been any strong link shown in studies between low glutamine and illness/immune compromise in athletes specifically.
There is also a small amount of research that has shown chronic changes to skeletal muscle glycogen, urea, C-reactive protein, creatine kinase, creatinine and iron levels.
Nervous System Response
The nervous system is affected significantly in overtraining syndrome, and is likely the key system responsible for the changes seen in the overtrained athlete (considering all organs and process within the body are driven by the nervous system).
The nervous system is split into two parts - the sympathetic (flight or fight) and parasympathetic (rest and digest) - which research has shown can be affected differently in different cases of overtraining.
Parasympathetic overtraining is associated with high volumes of aerobic/cardiovascular activity (i.e. running, swimming, cycling) and often leads to decreased resting heart rate and resting arterial pressure, low energy, extended sleep duration and depressive symptoms.
Whereas, sympathetic overtraining is more commonly associated with anaerobic system and strength/power dominant training (i.e. rugby, sprinters/jumpers, power lifters). This often presents with an increased heart rate and arterial pressure, decreased appetite and body mass, sleep disturbance and unusual restlessness/irritability or excitability.
Psychological and behavioural changes are, nonetheless, common in all serious cases of overtraining syndrome. Among physical symptoms, overtrained athletes also often experience apathy and lack of motivation, lack of confidence, inability to relax, loss of appetite, sleep disturbance (as mentioned above), irritability, depression and high self-reported stress levels.
All the outlined effects above are thought to be heavily influenced by brain neurotransmitters (such as Serotonin) as well as pro-inflammatory mediators (such as Cytokines). It’s also suggested that overtraining results in chronically decreased circulating Branched Chain Amino Acids as well as increased Tryptophan levels (a precursor to Serotonin). These effects can set off cascades of alterations to Hypothalamic - Pituitary - Adrenal Axis (HPA) and the Sympathetic - Adrenal -Medullary Axis (SAM).
While the scope of this article probably doesn’t warrant explaining in depth how these systems are affected in overtraining syndrome - we know that the global effects of prolonged stress exposure can manifest into nervous system changes in both pathways , and often leads to symptoms affecting more than just purely physical performance.
What actually happens to performance ?
As mentioned above, a hallmark feature of overtraining syndrome is performance decrement, particularly with an increase in training load.
Performance detriments of ~10% along with being unable to maintain regular training loads are not uncommon features in the overtrained athlete. For example, in overtrained distance runners specifically, 6-17% reduction in running pace during competition and 43-71% reductions in training distances have been reported.
In Judo athletes, a study found that some performance measures decreased before other symptoms of overtraining presented and suggested that performance monitoring could be a method for early detection of overtraining syndrome.
In elite QLD swimmers, it’s been shown that lap times slow down by up to 4% in those that demonstrated symptoms of overtraining sydrome. However these athletes actually had increased muscle soreness, perceived fatigue and poorer sleep quality well before performance decreases were evident.
While there are some differences in the research findings that could be related to many factors (especially differences in sporting demands), there are consistently clear detriments to performance in the overtrained athlete. What the research has told us, is that there are ways to identify overtraining syndrome early and intervene with the appropriate Exercise Physiology, Sport Science, Physiotherapy or Sport’s Medicine management.
What can you do?
Good quality sports rehabilitation and performance management should involve strategies to reduce the risk of overtraining a well as have systems in place to manage the symptoms of overtraining syndrome once present.
Guidance from an Exercise Physiologist, Sport Scientist or Sport’s Physician to take the following considerations into account can often be the defining point of difference between the sub-optimal and peak performance.
The 5 areas outlined below are evidence based methods that are thought to be effective for high performance athletes, however consulting your doctor before trying any new recovery strategies is still advised.

1. MONITORING
Despite having no single test that can screen or detect overtraining syndrome - there are a number of clinical and laboratory tests that can build a picture of athlete load tolerance, and subsequent risk for overtraining. The simplest way of effectively collecting information on this, is through self-monitoring and analysis of logbooks that include:
Training details/parameters (frequency, intensity, duration, type),
Competition/match play confidence/readiness,
Wellbeing (mood, energy levels, stress, fatigue, sleep quality, muscle soreness),
Causes/driver of stressors and dissatisfaction,
In females menstrual cycle/ pattern abnormality or irregularity
Other seasonal-type symptoms
Other comments of athletes training enjoyment/coping/emotional response
Testing generic blood markers of inflammation associated with immune stress (such as White blood cells, Neutrophils, T-Cells, Natural Killer Cells) could be performed in the chronically overtrained athlete, although there isn’t enough research to show that abnormalities directly increase the risk of overtraining.
Changes to blood Lactate responses during and post-exercise have been linked to overtraining. Considering there are so many variables that can influence normal Lactate fluctuation that regular / frequent testing of these markers and looking at changes over time is the only effective way to use this information in managing overtraining syndrome risk.
While self monitoring not practical, having blood Lactate threshold/exercise testing performed at regular intervals in the year/season with a Sports Scientist can be a useful way to monitor performance as well as detect changes that do related to overtraining.

2. MEDICAL
Combined with the monitoring approaches above -from a medical perspective, it is important to rule out genuine illness that can masquerade with overtraining-type symptoms of chronic tiredness and fatigue.
This is where investigations may be of the most importance (compared with screening for overtraining syndrome or monitoring biomarkers as risk factors), for example:
cardiac and lung health screening,
routine blood testing,
selective blood testing (for vitamins and minerals)
urine testing,
and serology for specific diseases (Epstein-Barre, HIV, hepatitis, Cytomegalovirus)
If other medical conditions are ruled out and a period of rest/training load reduction doesn’t help the athletes’ fatigue and performance, it’s much more likely that the athlete has a severe case of overtraining syndrome. In these cases, it can take weeks - months of further rest, nutritional/dietary modifications and high quality psychological support systems to fully recover.

3. NUTRITION/ERGOGENIC AIDS
Protein
1.2-1.7g/kg bodyweight per day - broken up into 20-30g regular servings thought the day is optimal to ensure a positive availability of energy, amino-acids and positive nitrogen balance for sufficient protein metabolism and optimal tissue repair.
The evidence for further intake above this amount with additional protein supplements of isolated/combined amino acid blends is not highly convincing and thus not recommended.
Carbohydrate
30-60g carbohydrate per hour during prolonged, sustained exercise
Immediately post-exercise approximately 1.0-1.2g/kg bodyweight should be consumed depending on the nature/intenisty of the training session and duration before t end strenuous training session - this ensure adequate energy stored as glycogen is available in the muscles and liver in preparation for the next bout of exercise.
The train-low compete-high approach of restricting carbohydrates until competitive play is still utilised in some theft circles and sports however for the purposes of immune function and optimal recovery- this needs to be periodised carefully into a medium-long term training program or meso/macrocycle.
Hydration
Monitor body mass changes in response to training sessions or competition bouts to asses fluid balance changes and moderate intake accordingly (this has been mentioned briefly in a previous Recovery Strategies article).
More specific and accurate measures of fluid balance can be taken using Urine Specific Gravity or Urine Osmolality testing.
This is particularly important to monitor when training in unaccustomed temperatures and higher altitudes, where fluid loss is greater, or simply in periods where infection risk may be increased such as at training camps.
Iron
Serum Ferritin <30ng/mL (females) or <50ng/mL (males)
While iron deficiency in athletes can be common in long-distance endurance athletes (due to increased gastrointestinal and genitourinary blood loss as well as being further facilitated by the stereotypical high-energy/high-carbohydrate diets that often won’t account for adequate dietary iron intake) , it’s also a lot more likely to occur especially in females, growing adolescents and athletes who need to diet/cut bodyweight regularly for competition.
Antioxidants
Supplementation of anti-oxidants in the absence of any actual observable nutrient deficiency is not recommended.
0.25-1.0g/day of Vitamin C could be of benefit during periods significantly increased training demands to reduce the occurrence of upper-respiratory tract infections.
Consume a variety of nutrient dense fruits and vegetables with a range of colours and textures.
Vitamin D
Seasonal screening in athletes for deficiency can be useful , particularly for indoor sport athletes who are prone to deficits or those who have a family history of bone conditions.
Those training or playing predominantly indoors could consider supplementation with 1000-2000IU/day of Vitamin D3 (upto 4000IU daily if initially deficient).
Athletes should avoid excessive Vitamin D supplementation unless there is a grossly obvious deficit identified on blood analysis.
Colostrum
10-20g/ day could have a beneficial immune effect, particularly during periods of greatest upper respiratory tract infection risk (i.e. winter, training camps, prolonged/extended travel periods and/or competition) Colostrum is not recommended for athletes’ consumption by the World Anti Doping Agency (WADA) due to the inclusion of growth factors within its composition.
Probiotics
Recommended at least 14 days before overseas travel or strenuous competition periods.
Multi-strain probiotics combining species from Lactobacillus and Bifidobacterium (>1 billon CFU/day) may offer the best chance of immune modulation and protection especially with high training demands

4. EXERCISE & LOAD MANAGEMENT
While training load is arguably the area that is most important in managing overtraining syndrome - it is also one that is often managed the least effectively. The methods of monitoring athlete load are mentioned above however, this is only usual if appropriate modifications can be made in response to detecting higher risk.
Like most pathologies, injuries or detriments to performance - managing overtraining is a balancing act of athlete demands and athlete tolerance.
By following this general guideline - two ways to modify load are by changing:
EXTERNAL LOAD - ie the actual training parameters or FITT (frequency, intensity time or type of exercise). This usually follows the prescriptive rules of reducing one or more areas of the FITT in order to better organise the demands placed on an athlete in order to limit excessive stresses that are detrimental to performance. For example, performing progressive heavy strength training during the playing-season in hopes of gaining significant strength, speed or power while game-play or competition is ongoing is usually an ineffective endeavour - as the demands of competition are already high enough. This is why Pre-Season training is so crucial to developing a foundation before entering season - as the focus should shift towards performing at 100% during games, matches and competition rather than focusing on maximum efforts/constant progression in the gym. When external loads/demands are too high either competition or training load will need to be reduced to limit chances of overtraining.
or
INTERNAL LOAD (the amount of load/stress placed internally on the athlete’s body). This can be thought of in simple terms as how well the athletes’ tolerance is to exercise or load. Again, the crucial factor of pre-season or off-season training to build foundations develops this tolerance, so that even when incredibly high demands are placed on the athlete - they can handle it.
For example, an athlete who is used to comfortably running at 80% top speed on most days of the week on top of max-effort strength training will have much greater chance of tolerating similar loads during season - while the athlete who hasn’t developed this tolerance may undertake the exact same exercise program but encounter injuries, illness and performance detriments quickly due to being overly fatigued. This can manifest from a weak link (leg endurance, cardiovascular fitness, core stability, mental toughness, anxiety coping strategies etc) that eventually fails in response to what is intended to be a normal progressive training environment. Sometimes this can be focally managed before full failure/overtraining syndrome occurs by directly focusing efforts on bringing the weak link up to speed (eg., adding stress management techniques for anxiety or adding stretches/massage to chronically tight muscle groups). This is harder to do when loads are already high in multiple areas and will often require backing-off from more than one area to prevent further decline.

5. OTHER RECOVERY METHODS
Generally speaking, all athletes who are overtrained (even those with severe overtraining syndrome) can benefit from tried and true recovery methods such as rest, low intensity exercise and mindfulness/meditation strategies.
Depending on the type of symptoms experienced, however, there may be ways to individualise certain methods of recovery to gain optimal effects.
For example, sympathetic overtraining (described above) might respond better to parasympathetic-style recovery techniques including stretching, yoga, massage, water-immersion, meditation etc.
While parasympathetic overtraining might respond better to sympathetic-style recovery techniques including ice/contrast baths, electrical muscle stimulation, certain dry needling/acupuncture techniques, saunas etc.
Although based around reputable research, these are generalised guidelines and the use of any recovery method should be individually tailored to the athlete for best results.
Check out our Recovery Strategies article Part 1 and Part 2 for some more simple but effective recovery techniques.
Take Home Points
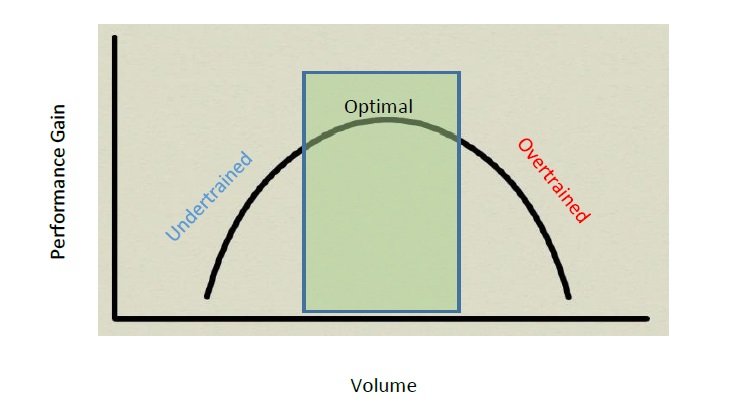
Overtraining Curve
Overtraining s a multifaceted clinical condition that can affect nearly all aspects of an athlete’s life.
Numerous contributing factors including training, nutrition, sleep and psychosocial health play key roles in the detection and management of overtraining syndrome.
While there are generic guidelines and strategies to reduce the risk of overtraining, the single most important factor that underpins ongoing performance improvements is having an individualised training program that is planned effectively.
While the adage ‘you can’t out-run a bad diet’ may be true regarding body composition, in terms of athlete recovery - there is definitely evidence to show that you can’t run away from bad programming.
No amount of shockwave therapy, dietary supplementation, massage therapy or ice baths can counter-act the detrimental effects of poor training programming.
If you’d like more information on any of the information above or would like a better understanding of how movement can be medicine for you, keep an eye out for more content like this or get in touch to book an appointment for a personalised plan of action today.